






A Chance to Improve Hepatitis C Care for PWID
Here is a review of an opportunistic treatment approach to HCV infection in this patient population in a European study and some of the potential challenges in applying it in the United States.

Marginalized populations, particularly people who inject drugs (PWID), are disproportionately affected by hepatitis C virus (HCV). In the United States, more than 80% of HCV infections are associated with injection drug use.1 With the use of highly efficacious direct-acting antivirals (DAAs), sustained virologic response (SVR) rates approach 100%.2 Thus, the World Health Organization goal to eliminate HCV infections by 2030 is theoretically achievable. However, previous literature demonstrated that SVR rates among PWID are significantly lower—as low as 20% in some studies.2,3 This can be attributed to previously well-defined and documented systemic- and individual-level barriers PWID experience in accessing, navigating, and remaining engaged in the health care system.4,5 Thus, investigators in the OPPORTUNI-C trial (NCT04220645) aimed to address disparities in accessing HCV treatment by evaluating the efficacy of opportunistic treatment of HCV infection among hospitalized PWID.6
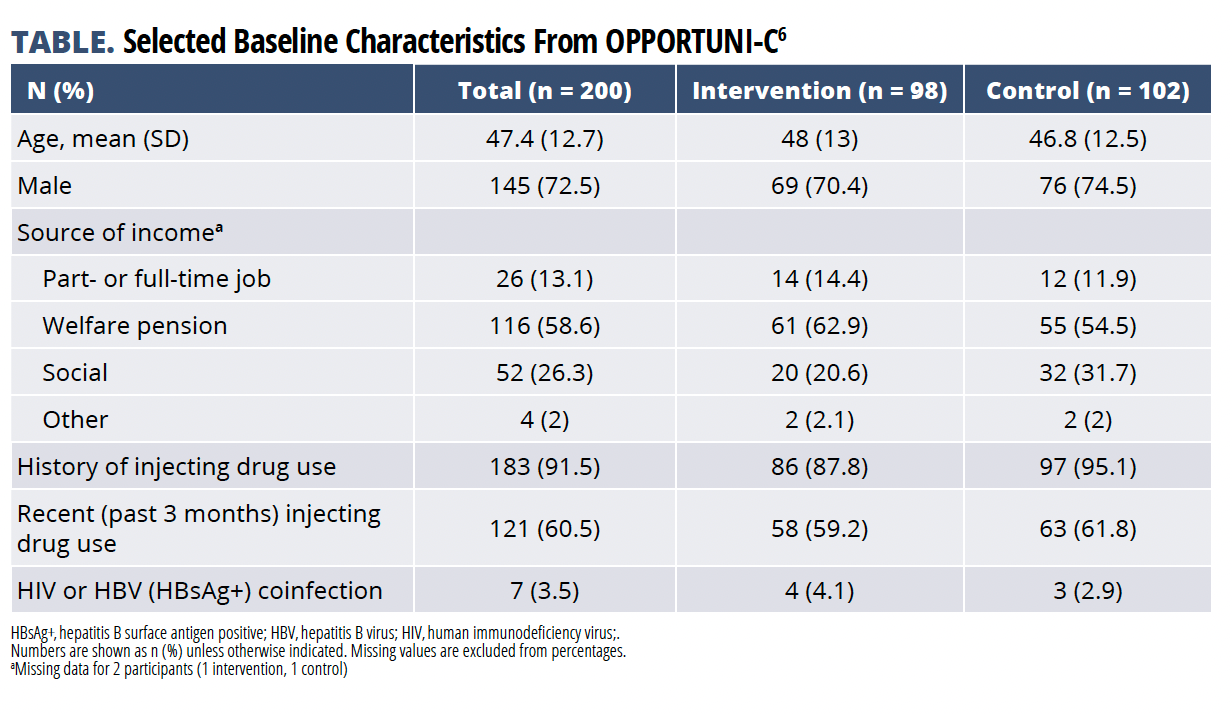
Midgard et al conducted the pragmatic, stepped wedge cluster randomized trial including individuals whose HCV RNA test results were positive and who were admitted for inpatient care at 3 hospitals in Oslo, Norway.6 Patients either received standard of care (referral to outpatient care) or intervention (immediate treatment initiation while hospitalized) conditions. The primary outcome was treatment completion, defined as the dispensing of the final package of prescribed DAA within 6 months after enrollment. Between October 2019 and December 2021, 200 individuals with positive HCV RNA results were enrolled.
The TABLE lists pertinent baseline demographics.6 Of note, 91.5% reported a history of injection drug use. Treatment completion was statistically superior with 68.4% completing therapy during intervention conditions vs 35.3% during control conditions [adjusted OR, 4.8; 95% CI, 1.8-12.8; P = .002]. Time to treatment initiation was statistically improved in the intervention conditions [adjusted HR, 4; 95% CI, 2.5-6.3; P < .001]; however, there was no difference in SVR rates at weeks 4 and 12 between groups. Based on the results, the investigators concluded that an opportunistic treatment approach to HCV infection in hospitalized PWID was superior to standard of care and should be further considered for broader implementation.


Although the authors discuss the strengths and limitations of their approach, application to clinical practice in the United States may be challenging to reproduce—a key element discussed in the accompanying editorial.7 Among the largest barriers to implementation are current Medicaid policies surrounding DAA coverage and prior authorization required for treatment.8 Currently, more than 25 states require prior authorization for DAA, with 10 states still enforcing a substance use restriction and/or counseling prior to treatment. This systemic inequity and discordance with HCV treatment guidance9 presents a large barrier to enacting rapid-start treatment for marginalized populations, especially PWID.
Midgard et al noted that 40% of patients with HCV were discharged prior to enrollment despite a median length of stay of 5 days, further emphasizing that even in a single-payer health care country, there likely are other systemic- or individual-level challenges that excluded patients from their study. Within the United States, we can presume that in addition to these challenges not described in the study, current DAA medication access and coverage limitations would add another layer of complexity in implementing this practice without additional mitigation measures.
This study also highlighted the challenges of keeping this patient population engaged in care. Week 4 and 12 SVR rates did not differ between the intervention and control groups, and the authors hypothesized this was due to missing SVR data (loss to follow-up) in the intervention group (21% intervention vs 4% control). Although the rate of dispensing the final DAA package was statistically higher in the intervention cohort, potentially inferring higher SVR rates than reported, the lack of patient follow-up for 21% of this cohort highlights and helps to quantify the magnitude of this challenge. Unlike caring for people living with HIV (PLWH), which requires lifelong antiretroviral treatment and continuous follow-up, patients with HCV have the opportunity to be cured in a relatively short period.9 Therefore, there is potential to learn from and apply some of the evidence-based systems in place to care for PLWH to PWID with HCV.10,11
Mobile community and other urban safety net clinics have demonstrated improvement in viral suppression in PLWH, including those with substance use disorder experiencing homelessness.11 The discussion surrounding how to better care for PWID who have HCV is relevant and current since US and international guidelines2,3,9 recommend treatment for all adults living with HCV infections, including people actively using substances. Thus, it is imperative we develop and implement novel strategies to provide access and consistent care to the highest-risk, and often marginalized, patient populations, specifically PWID. OPPORTUNI-C is a first step in ensuring we take advantage of the opportunity to treat all patients with HCV, undaunted by the potential challenges.
Highlighted Study
Midgard H, Malme KB, Pihl CM, et al. Opportunistic treatment of hepatitis C infection among hospitalized people who inject drugs (OPPORTUNI-C): A stepped wedge cluster randomized trial. Clin Infect Dis. Published online November 22, 2023. doi:10.1093/cid/ciad711
References
1.Morris MD, McDonell C, Luetkemeyer AF, Thawley R, McKinney J, Price JC. Community-Based Point-of-Diagnosis Hepatitis C Treatment for Marginalized Populations: A Nonrandomized Controlled Trial. JAMA Netw Open. 2023;6(10):E2338792. doi:10.1001/jamanetworkopen.2023.38792
2.World Health organization. Global Progress Report on HIV, Viral Hepatitis and Sexually Transmitted Infections, 2021. Accountability for the Global Health Sector Strategies 2016–2021: Actions for Impact.; 2021. Accessed January 2, 2024. https://www.who.int/publications/i/item/9789240027077
3.U.S. Department of Health and Human Services. Viral Hepatitis National Strategic Plan for the United States: A Roadmap to Elimination (2021–2025).; 2020. Accessed January 2, 2024. https://www.hhs.gov/hepatitis/viral-hepatitis-national-strategic-plan/index.html
4.Corcorran MA, Tsui JI, Scott JD, Dombrowski JC, Glick SN. Age and gender-specific hepatitis C continuum of care and predictors of direct acting antiviral treatment among persons who inject drugs in Seattle, Washington. Drug Alcohol Depend. 2021;220:108525. doi:10.1016/j.drugalcdep.2021.108525
5.Tofighi B, Sindhu SS, Lee JD, Chemi C, Leonard NR. Engagement in the Hepatitis C care continuum among people who use drugs. J Subst Use. 2020;25(4):343-349. doi:10.1080/14659891.2019.1704076
6.Midgard H, Malme KB, Pihl CM, et al. Opportunistic treatment of hepatitis C infection among hospitalized people who inject drugs (OPPORTUNI-C): A stepped wedge cluster randomized trial. Clin Infect Dis. Published online November 22, 2023. doi:10.1093/cid/ciad711
7.Rowan SE, Wyles DL. Don’t Put Off Until Tomorrow What You Can Do Today: Hospital Admissions as an Opportunity to Treat Hepatitis C. Clinical Infectious Diseases. Published online November 22, 2023. doi:10.1093/cid/ciad712
8.National Viral Hepatitis Roundtable, Center for Health Law and Policy Innovation of Harvard Law School. Hepatitis C State of Medicaid Access. Published 2023. Accessed January 2, 2024. https://stateofhepc.org
9.AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. Accessed January 2, 2024. http://www.hcvguidelines.org.
10.Christopoulos KA, Grochowski J, Mayorga-Munoz F, et al. First Demonstration Project of Long-Acting Injectable Antiretroviral Therapy for Persons With and Without Detectable Human Immunodeficiency Virus (HIV) Viremia in an Urban HIV Clinic. Clinical Infectious Diseases. 2023;76(3):e645-e651. doi:10.1093/cid/ciac631
11.Imbert E, Hickey MD, Clemenzi-Allen A, et al. Evaluation of the POP-UP programme: a multicomponent model of care for people living with HIV with homelessness or unstable housing. AIDS. 2021;35(8):1241-1246. doi:10.1097/QAD.0000000000002843




























