Are We at a Breaking Point for Adoption of Updated Susceptibility Interpretive Criteria?
The implementation of new College of American Pathologists rules presents an opportunity for collaboration between clinical microbiology laboratories and infectious disease pharmacists and physicians.



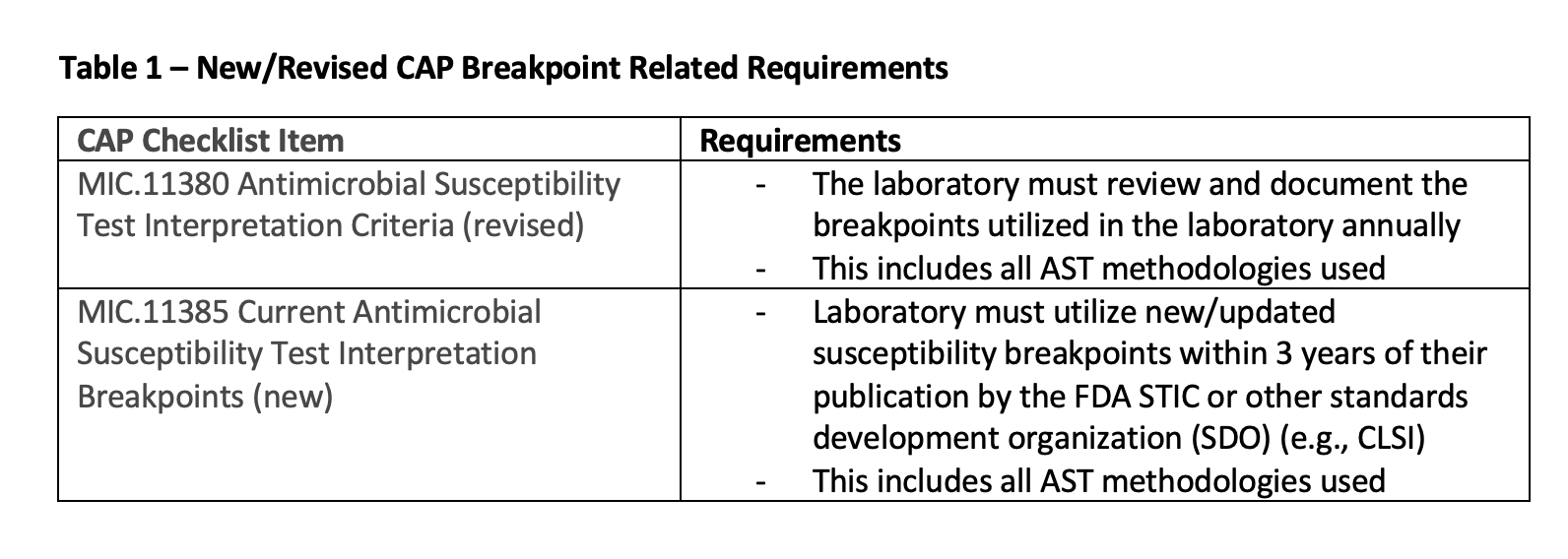
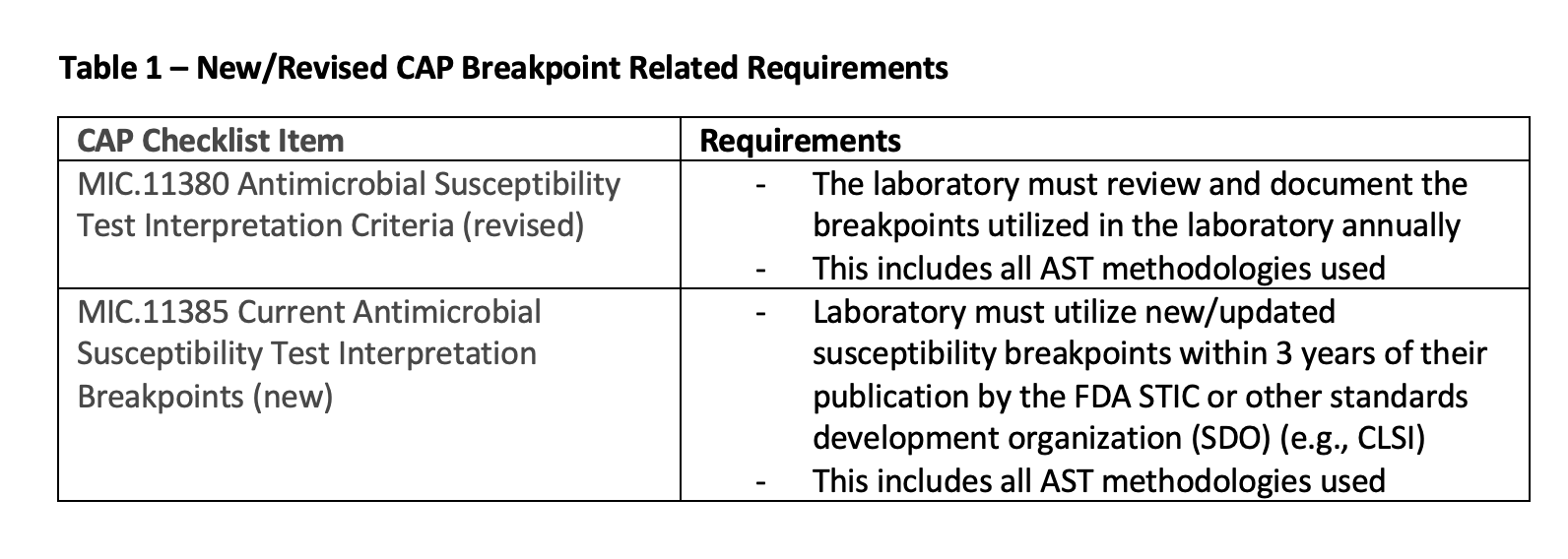
The seasons are changing, and for clinical microbiology laboratories in the United States, change is also coming. The College of American Pathologists (CAP) has modified one inspection checklist rule and added another related to antimicrobial susceptibility testing (AST) that will go into effect on January 1, 2024.1 The rules (Table 1) will require microbiology laboratories accredited by CAP to review and update their breakpoint interpretive criteria annually and implement new/revised breakpoints within three years of their publication (FDA, Antibacterial Susceptibility Test Interpretive Criteria [STIC], Clinical and Laboratory Standards Institute [CLSI] or European Committee on Antimicrobial Susceptibility Testing [EUCAST] breakpoints are acceptable).1,2

The practices outlined in the CAP rules may seem straightforward and be something most clinical microbiology laboratories already do, but unfortunately, that is not the case. As a part of a routine CAP survey competency assessment sent to laboratories in 2019, Simner et al. included a qualitative survey asking laboratories about their current AST practices and breakpoint use.3 The findings from this survey demonstrated that only 61.7%, 59.3%, and 62.2% of approximately 1,000 US laboratories who responded had implemented the ceftriaxone, ceftazidime, and meropenem Enterobacterales 2010 CLSI breakpoints, respectively.
The findings were also similar for implementing the 2012 CLSI P aeruginosa piperacillin/tazobactam breakpoint, with approximately 53% of responding laboratories having implemented the new breakpoint. Of the 56% of respondents who reported they had no ongoing projects to implement updated breakpoints, the most common reasons for inaction were manufacture-related issues (50%), staff/time/organism/cost-related resource limitations (24%), and lack of awareness of the need to update (12%).
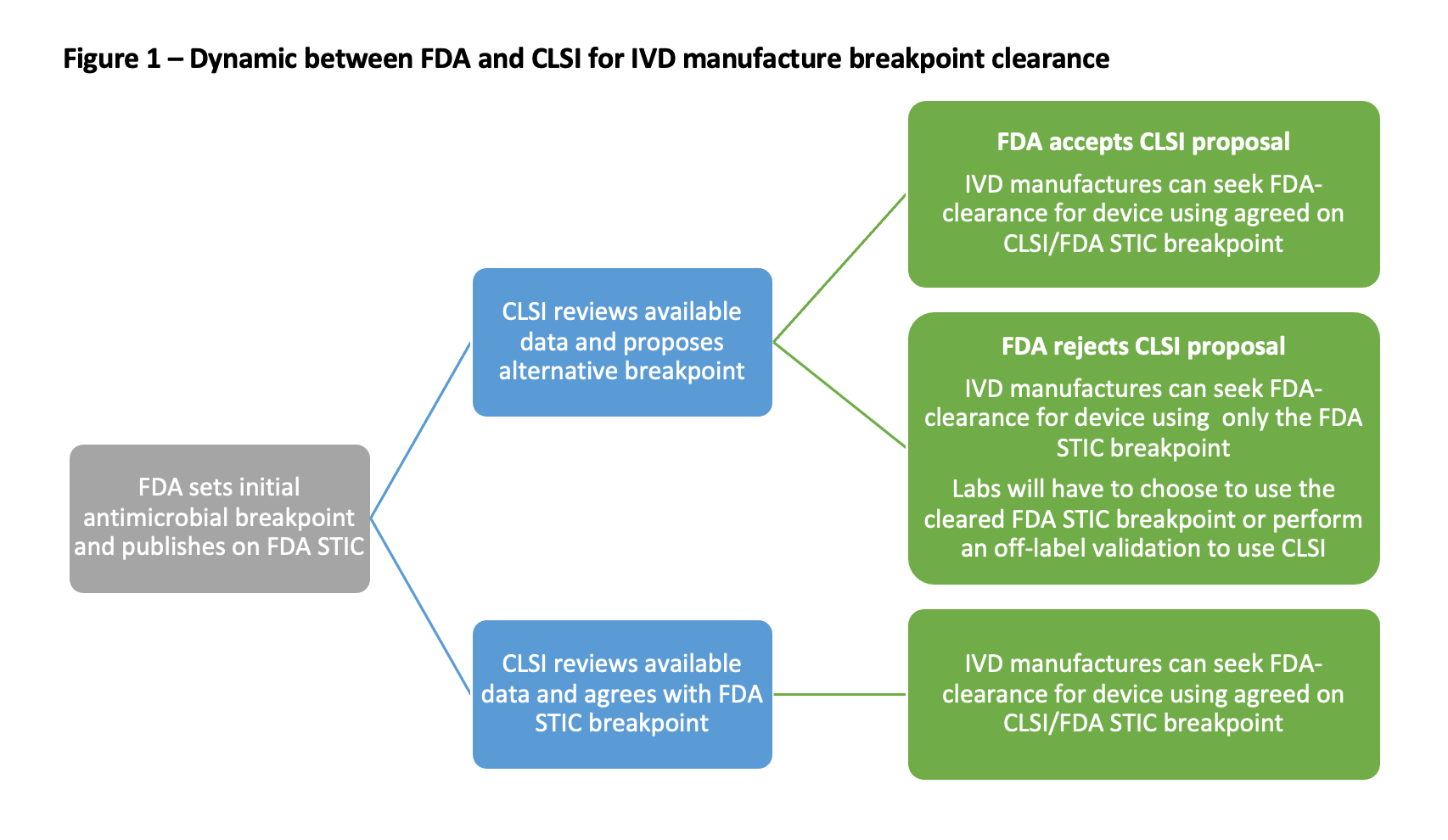
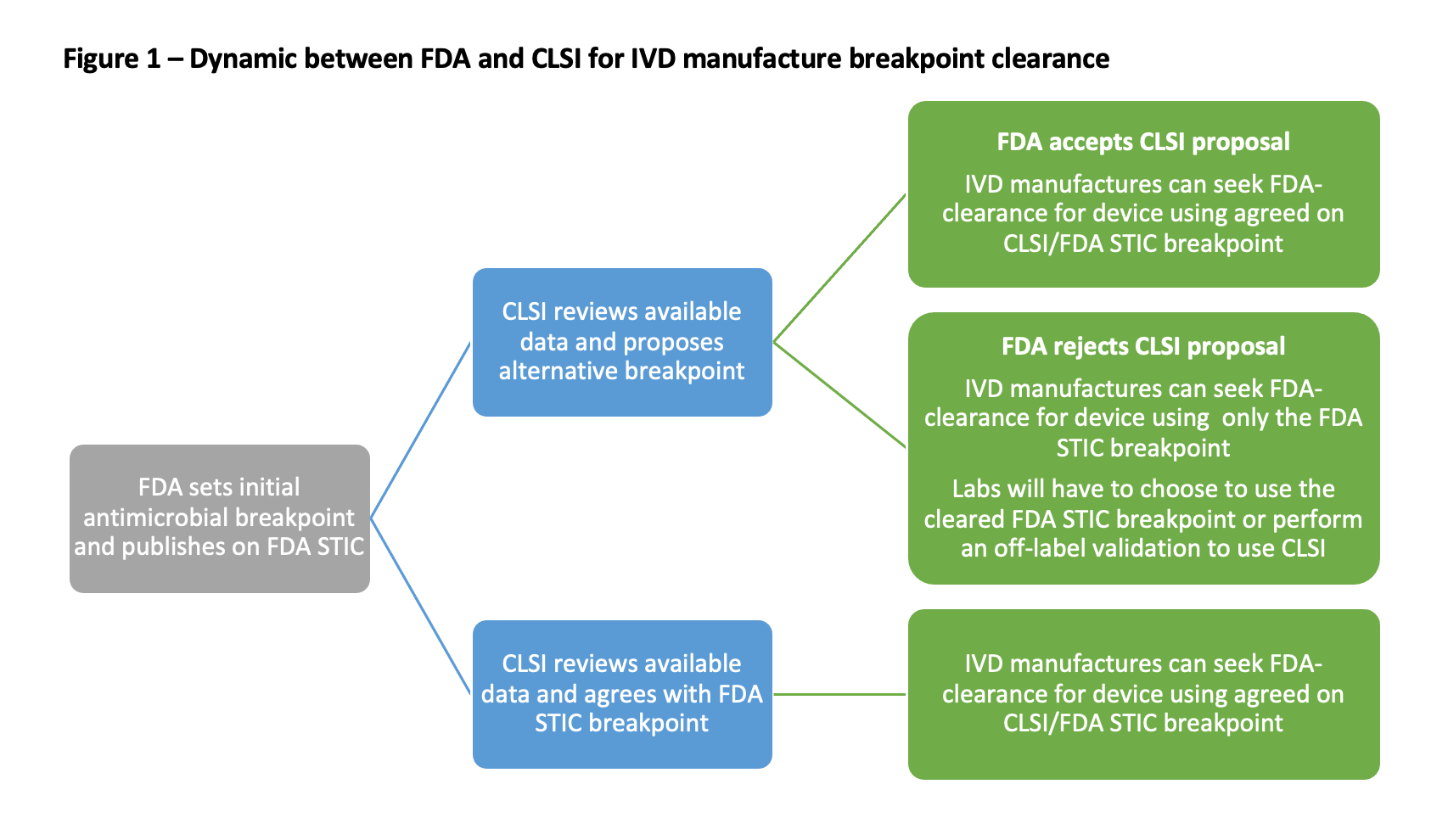
The manufacture-related issue is perhaps the most challenging to digest and address, given the complexity of microbiology in vitro diagnostic (IVD) regulation in the United States.4 The most common misunderstanding by clinicians and clinical laboratorians is that manufacturers follow the interpretive breakpoints published by the CLSI (eg, M27, M45, M100).5-7 However, AST manufacturers can only obtain FDA clearance for breakpoints published on the FDA STIC, for those organism species listed in the antimicrobial package insert (eg, cefazolin can only be FDA-cleared for Escherichia coli [E coli] and Proteus Mirabilis) under current regulations (Figure 1).8,9 Historically, this wasn't always the case, and pre-2007 AST manufacturers could pursue clearance based on both FDA and CLSI breakpoints in the US.
Susceptibility testing approved before this change was grandfathered, and manufacturers were allowed to maintain their prior clearance. This two-tiered system is why AST devices with broader label indications may be encountered. If manufacturers choose to seek updates to a pre-2007 test (eg, change the antimicrobial calling range, or implement new breakpoints), the revised test is subject to the post-2007 rules. Susceptibility device manufactures are not obligated by the federal government to update ASTs once they are approved, but the FDA is encouraging updates by the implementation of Breakpoint Change Protocols (a streamlined review process strictly for breakpoint changes implemented in 2019).4
Today, clinical laboratories are left with the conundrum of choosing between the FDA-cleared breakpoints for an AST or considering off-label testing to enable the use of CLSI breakpoints. Clinical laboratories can choose to pursue off-label (eg, utilize updated CLSI breakpoints, test additional organisms) testing of an FDA-cleared AST. However, before implementing off-label testing on patient specimens, the laboratory must conduct a validation study (typically ≥30 isolates per antimicrobial modified) to ensure acceptable testing performance.10-12 This testing may be beyond the resources of many clinical microbiology laboratories and was a commonly cited reason in the Simner et al. survey for why breakpoints were not up to date.3 The 2024 CAP checklist rules are contributing to changes in resource utilization priorities for many clinical laboratories. CAP-accredited laboratories (approximately 40% of US clinical laboratories) are actively evaluating the breakpoints they are using currently and which need to be updated to comply with the CAP checklist.4 Additionally, the CAP rules have also stimulated manufacturers to seek updated breakpoint clearances for their products, develop tools to help labs identify where gaps in CAP compliance might be, and, in some cases, develop new testing options (eg, redeveloping AST panels).13

For ID pharmacists, ID physicians, and other clinicians, the implementation of breakpoint update rules means that your microbiology laboratory is likely actively working through reviewing their currently in-use breakpoints and would appreciate the perspective of what matters to clinicians utilizing the data generated by the laboratory (eg, which breakpoint updates should be prioritized or de-prioritized, which antimicrobials are used frequently or not on the facility formulary). The process of ensuring CAP compliance also offers clinical teams the opportunity to dip their toes into stewardship efforts involving the laboratory and start building a robust ongoing relationship with the microbiology laboratory team for diagnostic stewardship projects if they have not already done so.14-16
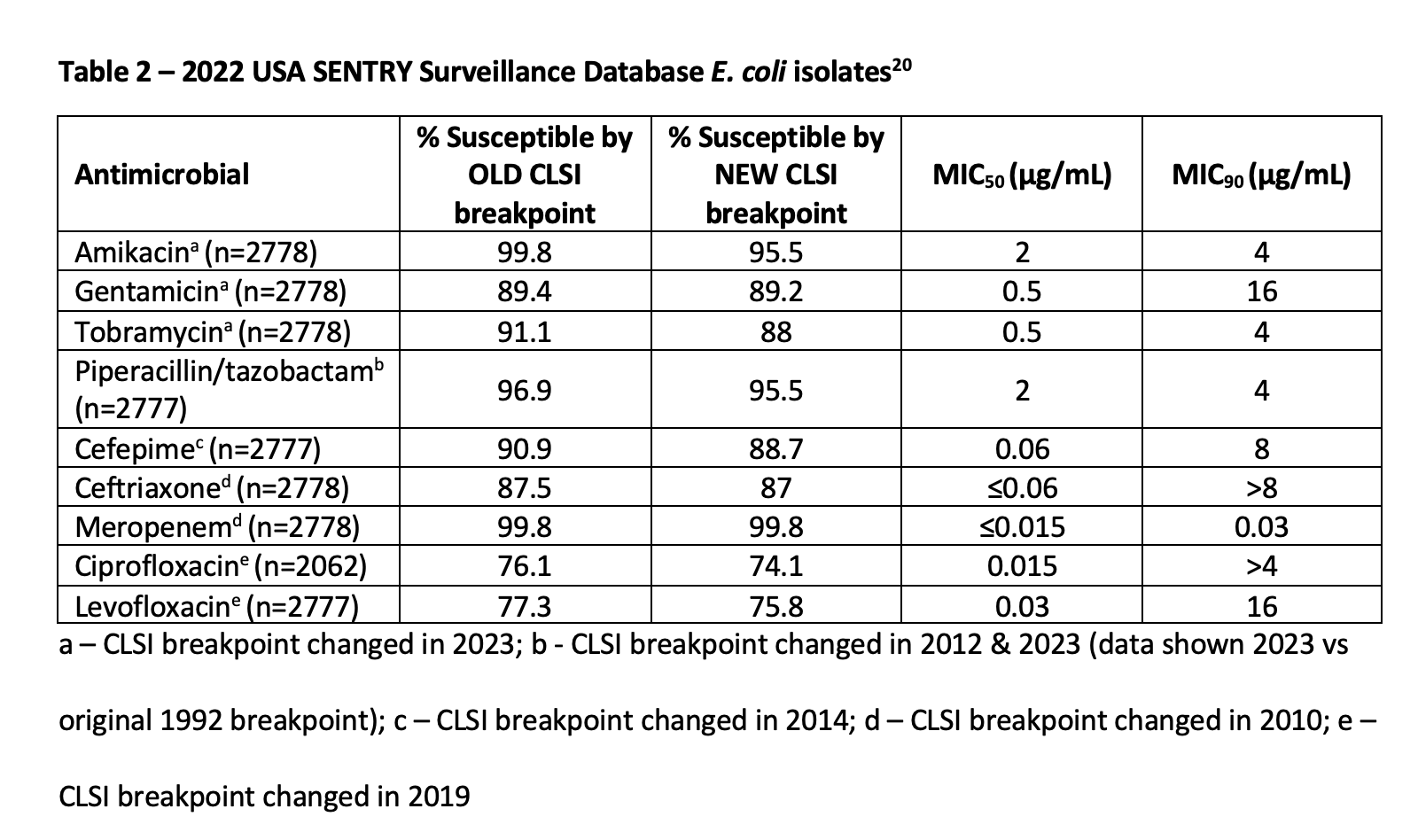
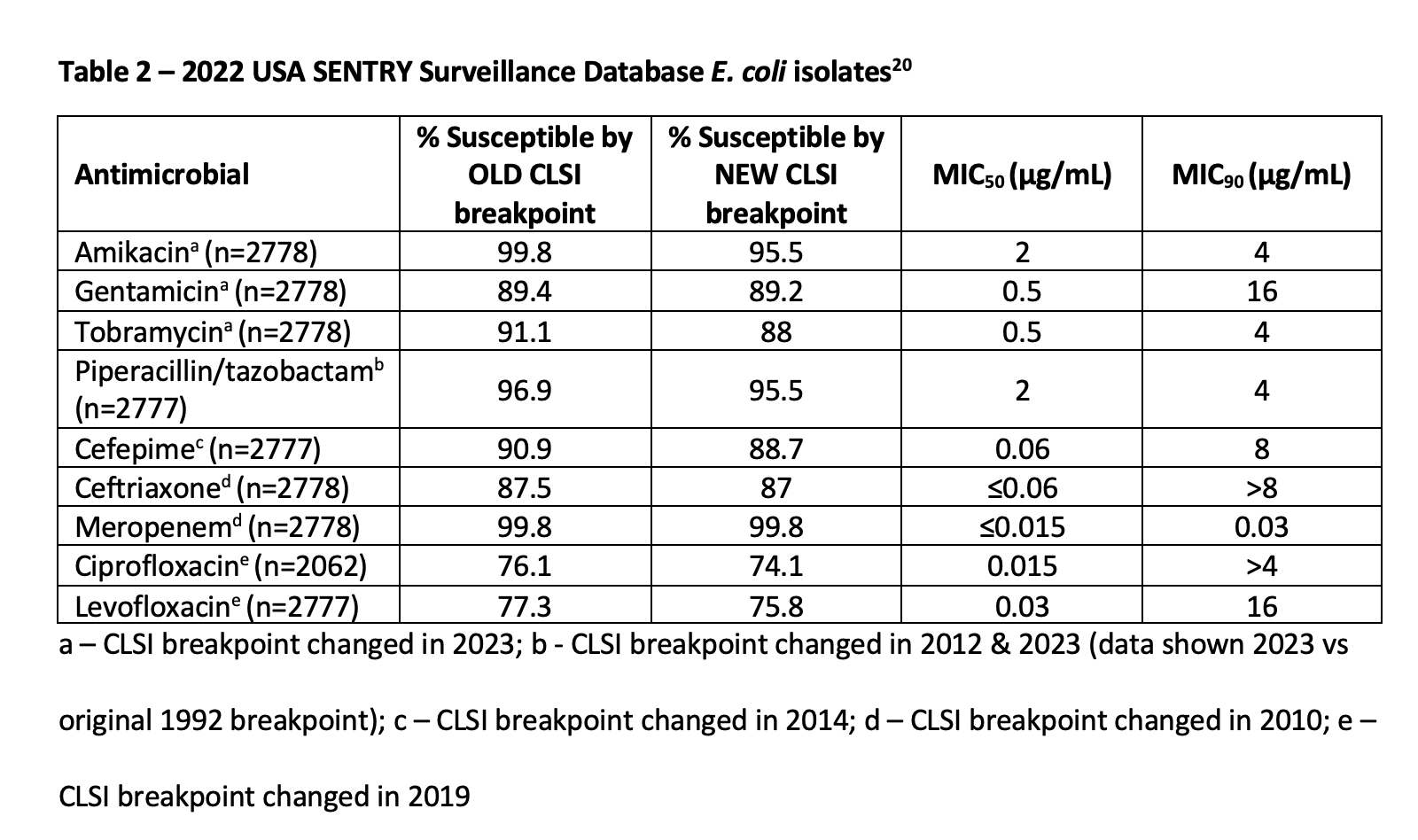
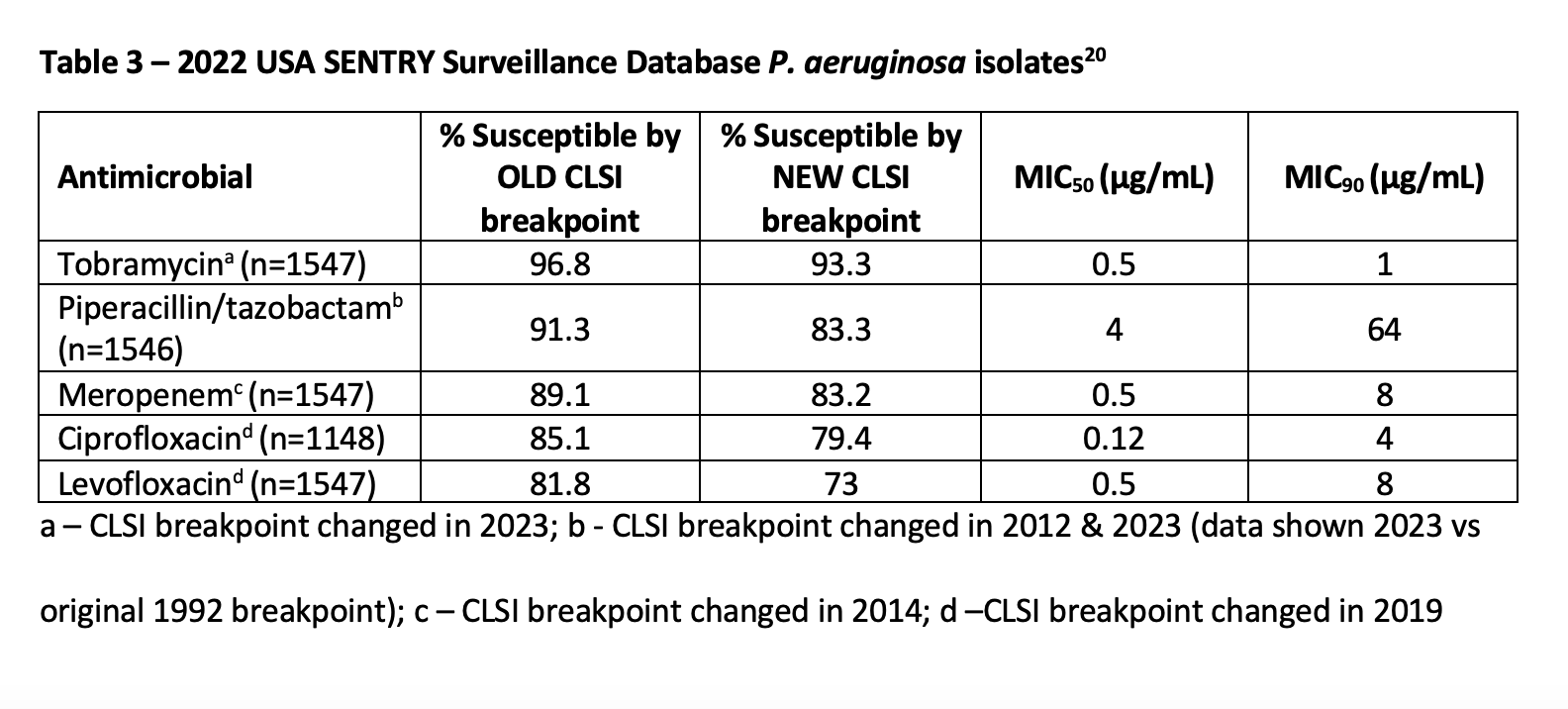
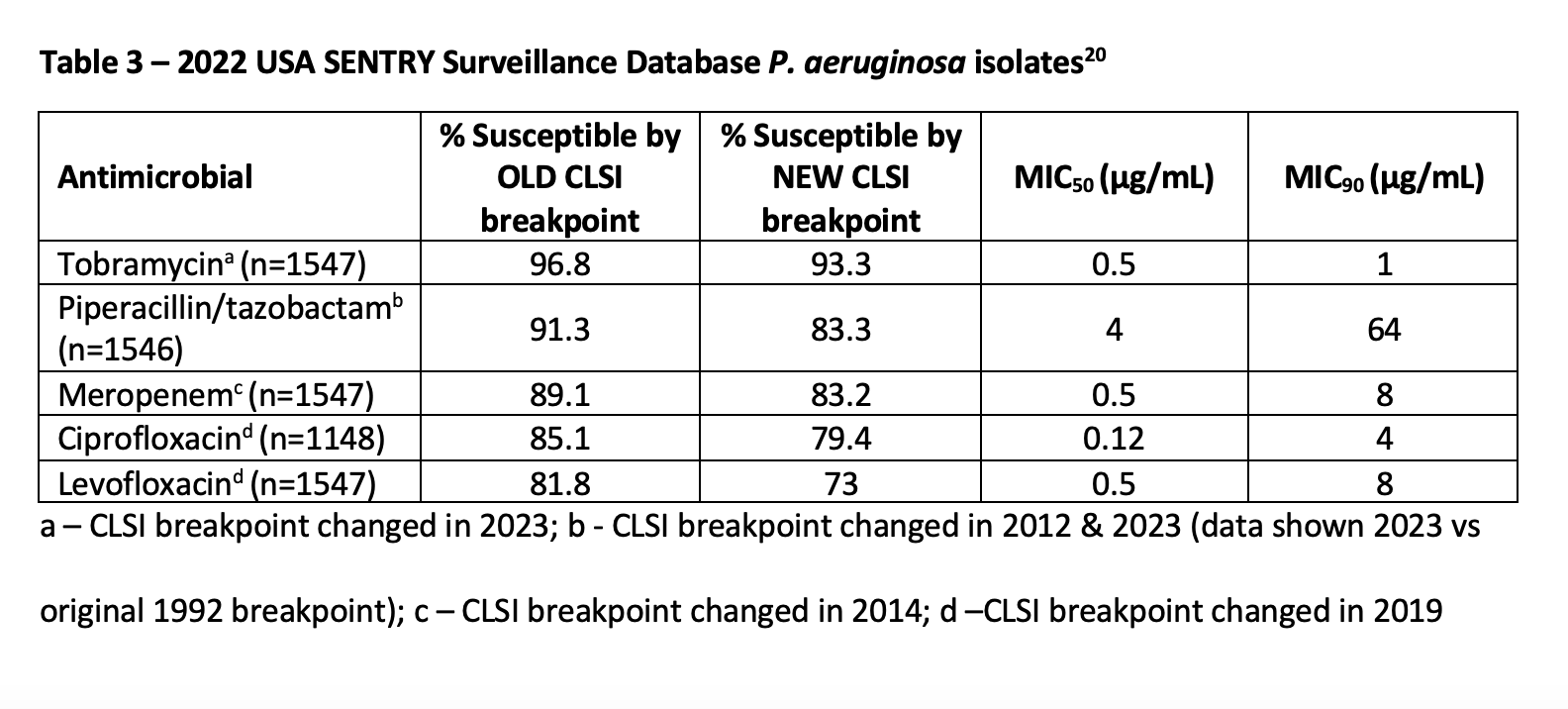
From an antimicrobial stewardship perspective, clinicians must also be aware that implementing revised breakpoints will result in changes in their antibiogram(s). These changes can range from minimal to radical depending on the breakpoints updated and the local organism epidemiology.17 For example, Van et al reported that approximately 4% of Enterobacterales and 10% of P aeruginosa in the SENTRY surveillance program collected in the US from 2011-2013 would have been reported as susceptible by the pre-2019 CLSI quinolone breakpoints and would now be considered resistant with the revised breakpoints applied.18 In 2018, Humphries et al reported that among 237 Enterobacterales harboring a carbapenemase gene, a significant number of isolates tested susceptible to imipenem and meropenem by the pre-2010 breakpoints (10.5% and 17.7%, respectively) vs interpretation with the post-2010 breakpoints (0% and 2.9%, respectively).19 Importantly, the impact of breakpoint updates is not always so profound. The SENTRY surveillance program data from isolates collected in the US during 2022 (Table 2, Table 3) provide an alternative perspective, driving home the importance of reviewing local data at each facility to understand and manage the potential impact.20 Centers may also have to consider analyzing the impact on particular sites of infection (eg, urine, blood) as they work to update facility-specific treatment algorithms and guidelines.


While we are entering a potentially difficult season preparing for CAP checklist compliance, especially for those working in clinical microbiology laboratories, we are also on the cusp of great opportunities to improve patient care. These CAP checklist items will help laboratories and clinicians ensure they are using the most up to date susceptibility interpretive criteria, accurately identifying antimicrobial resistance, and treating patients with effective antimicrobial options. It is incumbent on all of us to help make the most of this unique time when so many facilities are updating breakpoints to maximize the benefits for public health and patient care.
References
1.Humphries R. Updating Breakpoints–New Developments from CAP. AST News Update. 2022. Published Aug 2, 2022. Accessed Nov 16, 2023.
2.College of American Pathologists CoAACCS, 2021 ed. Northfield, IL: College of American Pathologists; 2021.
3.Simner PJ, Rauch CA, Martin IW, et al. Raising the Bar: Improving Antimicrobial Resistance Detection by Clinical Laboratories by Ensuring Use of Current Breakpoints. Open Forum Infect Dis. 2022;9(3):ofac007.
4.Patel JB, Alby K, Humphries R, et al. Updating breakpoints in the United States: a summary from the ASM Clinical Microbiology Open 2022. J Clin Microbiol. 2023;61(10):e0115422.
5.Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. 33rd ed. CLSI supplement M100 (ISBN 978-1-68440-170-3 [Print]; ISBN 978-1-68440-171-0 [Electronic]). Clinical and Laboratory Standards Institute, USA, 2023.
6.Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antifungal Susceptibility Testing of Yeasts. 3rd ed. CLSI supplement M27M44S (ISBN 978-1-68440-162-8 [Print]; ISBN 978-1-68440-163-5 [Electronic]). Clinical and Laboratory Standards Institute, USA, 2022.
7.Clinical and Laboratory Standards Institute (CLSI). Methods for Antimicrobial Dilution and Disk Susceptibility Testing of Infrequently Isolated or Fastidious Bacteria. 3rd ed. CLSI guideline M45 (ISBN 1-56238-917-3 [Print]; ISBN 1-56238-918-1 [Electronic]). Clinical and Laboratory Standards Institute, 950 West Valley Road, Suite 2500, Wayne, Pennsylvania 19087 USA, 2016.
8.Antibacterial Susceptibility Test Interpretive Criteria. U.S. Food & Drug Administration. https://www.fda.gov/drugs/development-resources/antibacterial-susceptibility-test-interpretive-criteria. Updated May 25, 2023. Accessed Nov 16, 2023.
9.Cefazolin [package insert]. Deerfield, IL: Baxter Healthcare Corporation; 2019.
10.CLSI. Verification of Commercial Microbial Identification and Antimicrobial Susceptibility Testing Systems. 1st ed. CLSI guideline M52. Wayne, PA: Clinical and Laboratory Standards Institute; 2015.
11.Jorgensen JH. Putting the New CLSI Cephalosporin and Carbapenem Breakpoint Changes Into Practice in Clinical Microbiology Laboratories. J Pediatric Infect Dis Soc. 2012;1(2):169-170.
12.Prinzi A. Updating Breakpoints in Antimicrobial Susceptibility Testing. American Society for Microbiology. 2022. Published Feb 22, 2022. Accessed Nov 16, 2023.
13.Humphries R, Abbott A, Rice F, Tekle T. Get Current! Using the 2023 Breakpoint Implementation Toolkit to Update and Document AST Breakpoints. Clinical and Laboratory Standards Institute webinar. Oct 26, 2023. https://clsi.elevate.commpartners.com/products/get-current-using-the-2023-breakpoint-implementation-toolkit-to-update-and-document-ast-breakpoints.
14.Claeys KC, Johnson MD. Leveraging diagnostic stewardship within antimicrobial stewardship programmes. Drugs Context. 2023;12.
15.Hueth KD, Prinzi AM, Timbrook TT. Diagnostic Stewardship as a Team Sport: Interdisciplinary Perspectives on Improved Implementation of Interventions and Effect Measurement. Antibiotics (Basel). 2022;11(2).
16.Morgan DJ, Malani P, Diekema DJ. Diagnostic Stewardship-Leveraging the Laboratory to Improve Antimicrobial Use. JAMA. 2017;318(7):607-608.
17.Truong WR, Hidayat L, Bolaris MA, Nguyen L, Yamaki J. The antibiogram: key considerations for its development and utilization. JAC Antimicrob Resist. 2021;3(2):dlab060.
18.Van TT, Minejima E, Chiu CA, Butler-Wu SM. Don't Get Wound Up: Revised Fluoroquinolone Breakpoints for Enterobacteriaceae and Pseudomonas aeruginosa. J Clin Microbiol. 2019;57(7).
19.Humphries RM, Hindler JA, Epson E, et al. Carbapenem-Resistant Enterobacteriaceae Detection Practices in California: What Are We Missing? Clin Infect Dis. 2018;66(7):1061-1067.
20.SENTRY Antimicrobial Surveillance Program. JMI Laboratories. https://www.jmilabs.com/sentry-surveillance-program/. Accessed Nov 20, 2023, 2023.
Newsletter
Stay ahead of emerging infectious disease threats with expert insights and breaking research. Subscribe now to get updates delivered straight to your inbox.
















